Click here to download the poster of our annual report!
Kootenay Boundary Division Leadership Report
wraparound care for Child and Youth Mental Health patients, launching new resources to support chronic pain patients,
successfully piloting an in-clinic social worker, integrating a GP specialist into the Trail diabetes clinic and collaborative care rounds successfully reducing antipsychotic use in Residential Care.
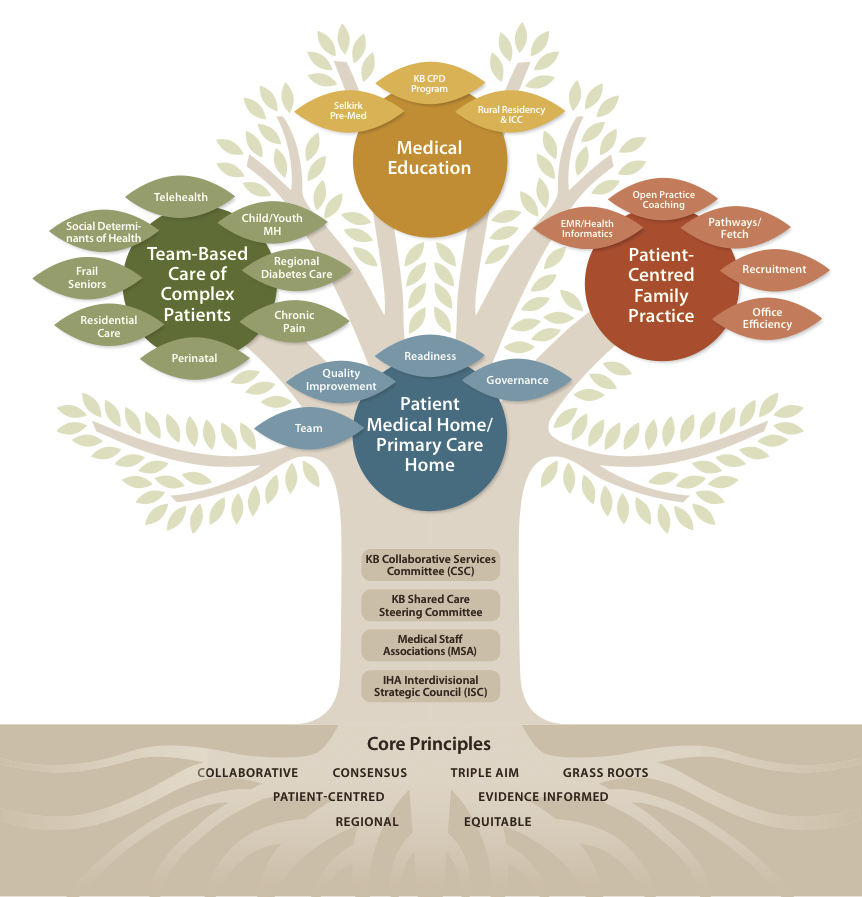
The dominant system change that will impact GPs on the ground continues to be primary care reform. Health Care is a complex system and no one is under any illusions regarding the pace of change or the complexity of interests at the table. However, implementation of the Patient Medical Home (PMH), robust team based care, and new GP-created funding models, are visible on the horizon. We remain optimistic that these changes will result in a more sustainable system, better patient outcomes, and richer more satisfying careers for physicians and NPs. Furthermore, your Division will be central to these conversations, representing your and your patient’s interests as change unfolds.
This year, the Division brought extensive KB Physician Leadership to primary care reform. Through the vehicle of the Collaborative Services Committee, we engaged with our members, IH staff, and community leaders, articulating the need for change and discussing new models of care that will work for Division members, members of the Primary Care Team, and KB patients. As this transformation evolves, it is clear there are complex and competing forces within the Ministry of Health, IHA, GPSC and Doctors of BC. The Division has worked to establish relationships with multiple leaders in these organizations, informing and influencing them regarding the direction and timing of change, keeping KB’s interests and the interests of all rural practitioners at the fore.
With this past year’s work as our foundation, the implementation journey begins. The KB Collaborative Services Committee has struck a working group that is approaching all KB clinics with an opportunity to initiate EMR-based Quality Improvement and Panel Assessment, a key first step in PMH implementation. Simultaneously the Group is analysing extensive demographic data regarding illness burden in each of our core sub-regions, and this data will be shared with our members. In addition, work is underway to develop systems for region-wide PMH Quality Improvement, and development of highly functioning Teams.
Notwithstanding the “bright shiny object” of the PMH, this year your Division continues to direct substantial resources to projects and programs that directly and immediately improve practice and patient care for every GP and NP in KB. CPD is offered at a high standard. Telehealth is expanding access to video consults to multiple specialities, and delivering secure texting (including enhanced RACE and hospital admittance/discharge notification). We anticipate bringing fully automated forms to every Intrahealth EMR in the region, and we are exploring doing the same for other EMR platforms. Open Practice Coaching remains available to all practitioners. We will maintain our commitment to robust support of physician recruitment, a fundamental foundation of sustainability of the profession in KB.
In this poster, you’ll find a summary of your Division’s work over the past year. A full write-up on all initaitives can be found at www.kbdivision.org/report2016. In particular, we draw your attention to the remarkable list of the GPs, NPs and partners, whose dedication to improving patient care in KB is evidenced by the countless hours they have dedicated to Division work. We thank you all, and look forward to a similarly productive 2016-17.
KB Division Executive:
Dr. David Merry, Chair
Dr. Lee MacKay, Physician Lead
Dr Trevor Aiken, Vice Chair
Andrew Earnshaw, Executive Director
Continuing Professional Development
Highlights for 2015-16 include:
-
Major CPD events: 33rd Kootenay Conference, Therapeutics Initiatives tour, AIME, HOUSE, Methadone, SEMP-SIM
-
More work as a region with KLH and KBRH hospital Rounds being accessed through video conference by remote sites, as well as more regional events than ever that are funded through multiple reverted CME funds
-
Division contribution of an additional $10,000 to support physician leadership in regional CPD events
-
$9,000 in additional funding from the REAP program, more than ever before
-
Introduction of new branding and templates to streamline communications to members
-
Better alignment with PSP’s and the KB Nurse Educators’ CPD offerings to minimize overlap and better promote all events
-
Expanded CPD distribution list, to include other health care practitioners (e.g. community pharmacists) to continue the efforts towards more interprofessional education
Regional Medical Educators
Many Division members bring leadership and preceptorship to KB’s Rural Residency and Integrated Clinical Clerkship programs, recognizing the vital role Medical Education plays in maintenance of the profession, and enhancement of the quality of patient care across KB. Selkirk College, with the active engagement of numerous Division members, has similarly risen to the challenge of fostering rural healthcare sustainability by launching a Rural Pre-Med program, the first cohort of which is applying for Medical School this year.
The Division actively supports both these initiatives. Financial Support is provided to the Rural Residency & ICC programs to support expenses outside the purview of UBC’s funding, with a particular focus on the tremendous unpaid contribution made to the program by its Faculty, and the increased costs associated with delivering a distributed program in a rural context. At this years AGM, we are launching a “matching dollar” program, supporting local Med Staffs who wish to make pooled donations to a Bursary for Selkirk Pre-Med students in financial need.
EMR/Health Informatics
In the spring the Division initiated a project focused on electronic medical record (EMR) systems integration in Boundary Region. The goal is to integrate the current five separate EMR systems to create a “single electronic medical record” for each patient that is accessible by all Boundary clinics and in the Boundary Hospital emergency department. This shared EMR solution will ensure the continuity of care for all Boundary residents. The direction is towards an Interior Health (IH) hosted shared EMR solution for the Boundary.
In the Summer we collaborated with IH to facilitate 4 workshops to help guide improvements in the EMRs and other electronic systems. Workshops were held in GF, Rossland, and Nelson bringing together various physicians, nurses, allied health, clinic staff and administrators to provide input and direction.
In the fall we Initiated two projects: (i) an EMR forms optimization project to increase the level of clinical efficiency through improved use of electronic forms within provider EMRs across the region, and (ii) Driving Clinical Value via Health Data Collaborative technologies with initial roll-out at Nelson Medical Clinic
Recruitment/Retention
The Division recruitment and retention program welcomed a new Project Manager for 2015-2016, with the continued mandate to lead recruitment and retention efforts by being the first point of contact for candidates and Division members.
Since the launch of the recruitment and retention program, 24 new primary care providers have been recruited and begun seeing patients in Kootenay Boundary. We have attended 5 events and built a list of over 100 residents and physicians interested in our region with multiple newsletters sent to date. We have organized and supported social events for residents and new GPs and provided assistance to 18 members needing recruitment support for their clinic. Our recruitment website has had almost 4,000 page views since launch and we have created a cost-effective facebook advertising campaign targeting GPs in key locations (Canada, US, UK and South Africa).
In late 2016 we will be part of the 2016 Health Match BC booth at the Family Medicine Forum in Vancouver and will continue our marketing efforts and support for Kootenay Boundary GPs and clinics through 2016-17.
Finally, a thank-you to all those who have supported the Division’s recruitment program through 2015-16.

PATIENT CENTRED FAMILY PRACTICE
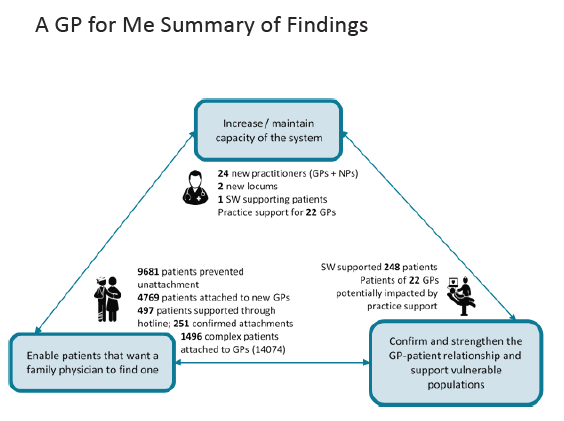
A GP For Me
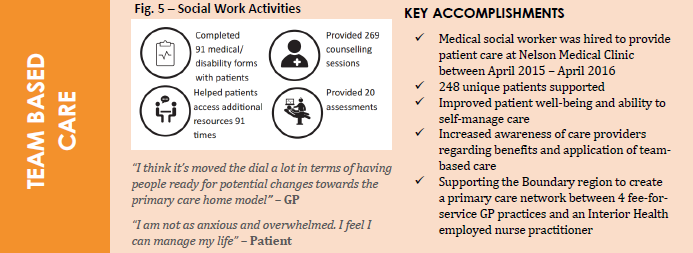
Team-Based Care - Social Worker
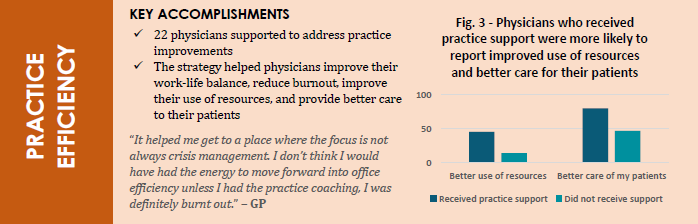
Improved Practice Efficiency
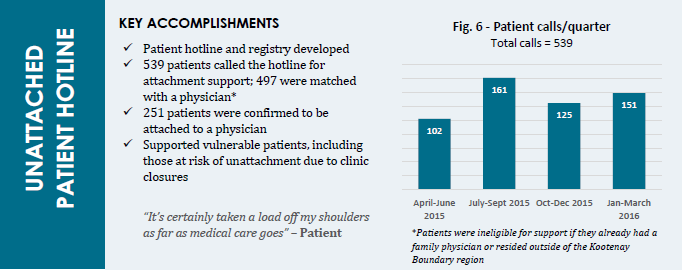
A GP for Me Hotline
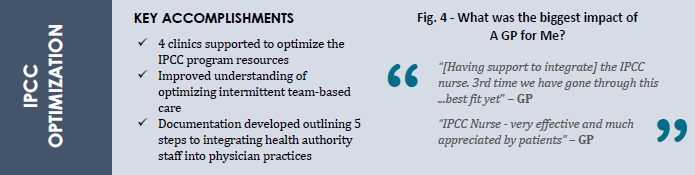
IPCC Optimization
Primary Care Home - Primary Medical Home
Through 2015-16, the Division has made its first priority to take a strong leadership role in supporting the strategic development and implementation plan for the Primary Care Home/Primary Medical home initiative introduced by the Ministry in spring 2015. The proposed changes are a paradigm shift in how primary care and indeed all health care will be delivered in the near future.
As soon as the Ministry papers came out in March 2015, we went to every medical staff meeting around the region to share highlights and encourage a full review of the papers by all GPs and NPs. In the fall, the Collaborative Service Committee (IH & Division) began positioning ourselves as an early adopter region and have been building strong relationships throughout the year with Ministry of Health, Health Authorities and GPSC leadership.
Around our November AGM in 2015, the Prince George Division and Northern Health Authority leadership toured the region to present their experience of implementing the Patient Medical Home in the north.
In the spring, the Division and our IH partners hosted over a dozen engagement events to explain the pressures motivating this change, how we hoped to bring local control to the process, and an outline of potential new resources that we anticipated will be introduced to support implementation.
CARE OF COMPLEX PATIENTS
Chronic Pain
KB Division has been working with our IH PSP colleagues as well as BC’s Pain BC on a number of initiatives in 2015-16 including:
-
Supporting the PSP Chronic Pain Module learning sessions in Trail
-
Launching Pain BC’s online ‘Live, Plan, Be’ self management tool in KB
-
Developing area specific chronic pain services directories (Lower Columbia complete, Nelson/area coming soon!)
Finally, KB Division and Pain BC are exploring the potential for virtual rounds/case conferencing learning sessions with provincial experts in 2016-17, as well as the creation of local ‘Pain Action Teams’ in KB communities to help raise awareness, provide support and drive improvements in chronic pain care at all levels.
Polypharmacy and Residential Care
The GPSC Residential Care Initiative’s MOU was signed in July 2015, leading to new funds now being available for KB GPs who are providing residential care in facilities. For the 2015-2016 fiscal, $116,806.25 was disbursed to 43 GPs. The Residential Care Initiative is continuing for the 2016-2017 fiscal and the funding does not have an end date.
A Division and IH team led by Dr. Trevor Janz is also actively implementing multi-stakeholder Quality Improvement processes throughout Kootenay Boundary. This initiative is attracting provincial attention for its’ use of Quality Improvement principles to improve residential care.
The region has seen dramatic declines over the past several quarters in the use of medication. All but two facilities were below the IH and BC average for nine or more medications in Q3 of 2015, and many facilities have shown a downward trend over the last several quarters.
Thanks to the innovative “Responsive Behaviours in Seniors Rounds Teleconference” which brings physicians, care teams and psychiatrists together on monthly calls to triage current patient cases and share best practices, Kootenay Boundary has seen antipsychotic use, once the highest in Canada, drop down to below the BC and IH average for all but one facility.
Quality improvement work will continue through 2016-2017 and we thank all those who have been involved in the polypharmacy and residential care projects this year.
Frail Seniors
Our work in 2015-16 has hinged on further developing relationships with our IH colleagues involved in Frail Seniors. A report was written through early 2016 and later this year, lead administrators from the portfolios will be making recommendations to the Collaborative Services Committee (IH and Division) regarding next steps.
Several professional team meetings have taken place between staff in acute/allied health and community portfolios with the objective of improving systems and processes relating to the discharge planning process for family physicians.
SOCIAL DETERMINANTS OF HEALTH
Poverty Intervention Tools
Since launching in 2014, the Poverty Tool has been adapted by multiple communities around BC. In early 2016, KB Division was approached to support development of ‘version 2.0’ of the tool at the provincial level by thewellhealth.ca organization. The updated tool is expected to be available for practitioners in the fall of 2016.
In the spring 2016, KB Division with the support of Blue Cross hosted a province wide day long event in Vancouver discussing physician leadership in the Social Determinants of Health. The entire afternoon was dedicated to exploring what collective action on SDH might look like in BC. Next steps that will be actioned through 2016-17 include:
-
Creating an interdivisional network for addressing SDH supported by the Provincial Division Office.
-
Initiating universal poverty screening in all GP practices, integrating this into EMRs.
-
Advocating at local municipalities for a provincial poverty reduction strategy. (BC Poverty Reduction Coalition provides an action toolkit.)
-
Creating a toolkit for integrating SDH into Primary Care Home practice.
SPECIALIST/GP COLLABORATION
Child/Youth Mental Health Substance Use
This year, members of the Child and Youth Mental Health and Substance Use - West Kootenay and Boundary Local Action Teams (LATs) have worked to develop an in-depth understanding of shared context, values and foundations to ensure child and youth mental health and substance use services in the Kootenay Boundary region are family and culture centred, responsive and collaborative.
Some key practice implications for this work include:
- Seeking out and facilitating family, extended family and community participation;
- Working together in a way that honours and respects all perspectives, and recognizes the sharing of decision-making and responsibilities;
- Ensuring there is shared access to information in a transparent manner;
- Recognizing the importance of connections to community and culture, and encouraging and facilitating those connections;
- Utilizing trauma-informed approaches and understanding the impact of inter-generational trauma on youth, families and communities.
West Kootenay Local Action Team:
In September 2015, the Kootenay Boundary Division of Family Practice and the West Kootenay LAT engaged Dr. Barry Trute who resides in Nelson BC. Dr. Trute served as ARC Professor of Family Centred Care at the University of Calgary, holding joint appointments in Social Work, Nursing and Paediatrics. His leadership in Canada in the development and advocacy of a Family-Centred Practice model in health and social services has been instrumental in supporting the West Kootenay LAT to implement a Wraparound service test model in the region.
Results from these Wraparound tests have shown improvements for youth and their families including reduced visits to the Emergency Room, reduced suicide risks and improved school relationships. This work will continue in 2016/2017 with the addition of a Wraparound Resource Coach and a Parent Coach who will help support medical home, school and community Wraparound tests of change.
Boundary Local Action Team:
Since the inception of the Boundary LAT (December 2015), the team has undertaken a Patient Journey Mapping process with families with lived experience to identify gaps in services as well as services and processes that were found to be supportive.
Physicians, mental health and substance use service providers, and school staff have also been engaged in a “Meet and Greet” dinner in concert with the Practice Support Program Child & Youth Mental Health Module. The LAT has also trialled a Care Navigator test of change to identify barriers and challenges faced by children, youth and their caregivers who recurrently present at the Emergency Department of Boundary Hospital and/or in primary care settings in rural and remote communities for mental health and substance use concerns. The goals of the test of change are to learn about the challenges faced by these families and help facilitate connections between acute care and/or primary care services and mental health and substance use services in the community.
Pathways
In early 2016, all Kelowna specialists were added to the Pathways database. Now KB doctors and nurse practitioners can search for specialists in major referral centres across BC from Kelowna to the Lower Mainland. Thanks to the input of many KB physicians, links to multiple new resources have been added to KB Pathways including diagnostic imaging wait time information, thrombosis guidelines and ICD-9 codes among others. The Division has been touring the region to give tutorial sessions outlining the features on Pathways with the following results since launch:
-
Approximately 35% of KB practitioners using Pathways regularly
-
Over 1,519 specialist page views by practitioners
-
Over 370 physician resources downloaded
-
Over 100 forms downloaded
Tutorial sessions are still available to all Physicians, Nurse Practitioners and MOAs. Contact Paul - pedney@divisionsbc.ca.
Telehealth - RACE, ED-ICU Video Conference, Telehealth, Secure Texting
The Shared Care Telehealth project formally got underway in January this year and started off with a flurry of activity. Bringing together two digital care initiatives started in previous Shared Care projects, Tele-maternity and Rapid Access to Consultative Expertise (RACE), the Technology in Practice project expands on the opportunities to use in-clinic video conferencing for better patient care, and the adoption of secure texting for physician communications including RACE.
Key Accomplishments to date:
-
Hosted engagements with 35 physicians (family physicians and specialists) and Interior Health colleagues to meet new Chief Medical Information Officer Dr. Douglas Kingsford on the future of IT;
-
Engagements with 70 physicians (family physicians and specialists) to determine interest in secure texting system implementation;
-
Completed patient telehealth survey
-
Installed in-clinic secure video conferencing systems in 17 locations ~ 8 family physician clinics, 9 specialists;
-
Eight specialties engaged to provide video conferencing services for patients;
-
13 patients seen through video conferencing testing;
-
Implementation plan for secure texting developed for Fall 2016.
Regional Diabetes Care
Over the last year the Regional Diabetes Committee has been working in partnership with Interior Health to increase referrals to an enhanced GP/SP Shared Care model at the Trail Diabetes Education Centre (DEC). This project has resulted in better patient outcomes for individuals living with diabetes in the Trail area and surrounding communities (Rossland, Castlegar, Fruitvale, Montrose). Between January and June of 2016, over 150 new referrals were received at the Trail DEC and there was a 209% increase in the number of team appointments over the same period the previous year. Patients of the Trail DEC who had team appointments (with a GP or SP, nurse and dietitian) between January and August 2016 experienced a statistically significant decline in average blood sugar levels (HbA1cs), a key diabetes measure. 69% of patients experienced a decrease in HbA1c and the average decrease across the group was 0.83. 68% of respondents rated their experience at the Trail DEC a 10 on a scale of 1 to 10 and an additional 19% rated it a 9.
Maternity – Child
The Regional Perinatal Advisory Committee received new funding this year to achieve improvements in care for mothers who experience mental illness during pregnancy or post-partum. Three key goals are:
|
1. Work with key “entry points” to service to: develop standardized approach to screening and supporting new moms at risk of or with mental health challenges; improve attachment between moms and babes; reduce stigma about mental illness: 2. Revise mental health service intake process to recognize perinatal mental health referrals as a co-morbid condition and increase priority of patients for support 3. Develop skills of multi-disciplinary professionals for better screening, diagnosis, and awareness of treatment options for new mothers while building collaborative local service networks.
|
Key accomplishments:
-
Patient needs assessment about perinatal mental health supports in the KB;
-
MHSU revision of intake processes to improve response times for new moms:
-
Development of a referral pathway tool for perinatal mental health;
-
Series of workshops hosted by BC Reproductive Mental Health available for community organization groups facilitators, clinicians, and physicians;
-
Familiar faces program initiated in the Boundary region - cross professional interactions with new and expecting moms to normalize services and increase accessibility;
-
Familiar Faces program to expand into all four communities in coming months;
-
Pilot program initiated as a collaboration between MHSU and community organizations to provide group support sessions in four communities;
-
Interprofessional learning sessions to be provided in spring 2017.